Almost everyone has heard of autism. We’ve come a long way in raising awareness about it. But, the facts about autism and how it affects people, along with the history of the condition, are lesser-known.
I talk about autism a lot, so I’m going to go over some important information about autism here for those who are wondering what is autism, really?
This article covers:
What is autism?
In the past, autism was misunderstood and rarely discussed in public. Thankfully, a lot has changed, and we now have a better understanding of what autism truly is.
Autism Spectrum Disorder (ASD) is a “neurodevelopmental disorder that impacts brain development causing most individuals to experience communication problems, difficulty with social interactions, sensory processing differences, and a tendency to repeat specific behavior patterns. There is also a markedly narrow repertoire of activities and interests.” (Source) In other words, they tend to have particular special interests which may occupy a lot of their time.
The term “neurodevelopmental” means that it is related to the way the brain grows and develops. This means that although there are often challenging behaviors associated with autism, it is not a behavioral disorder.
In other words, children with autism don’t choose to behave in a challenging way – they behave in a challenging way because various lagging skills make them require additional supports to respond adaptively in various environments.
The term “spectrum” describes the wide range of challenges and abilities people with autism face. Since the effects are so broad, no two individuals have the same challenges.
The effects of ASD are lifelong impacting on all areas of a person’s life. Additionally, no two individuals with autism are alike and may have significant differences in skills across multiple domains. However, autistic individuals can and do often live very fulfilling lives.
Autism History
1910-1920
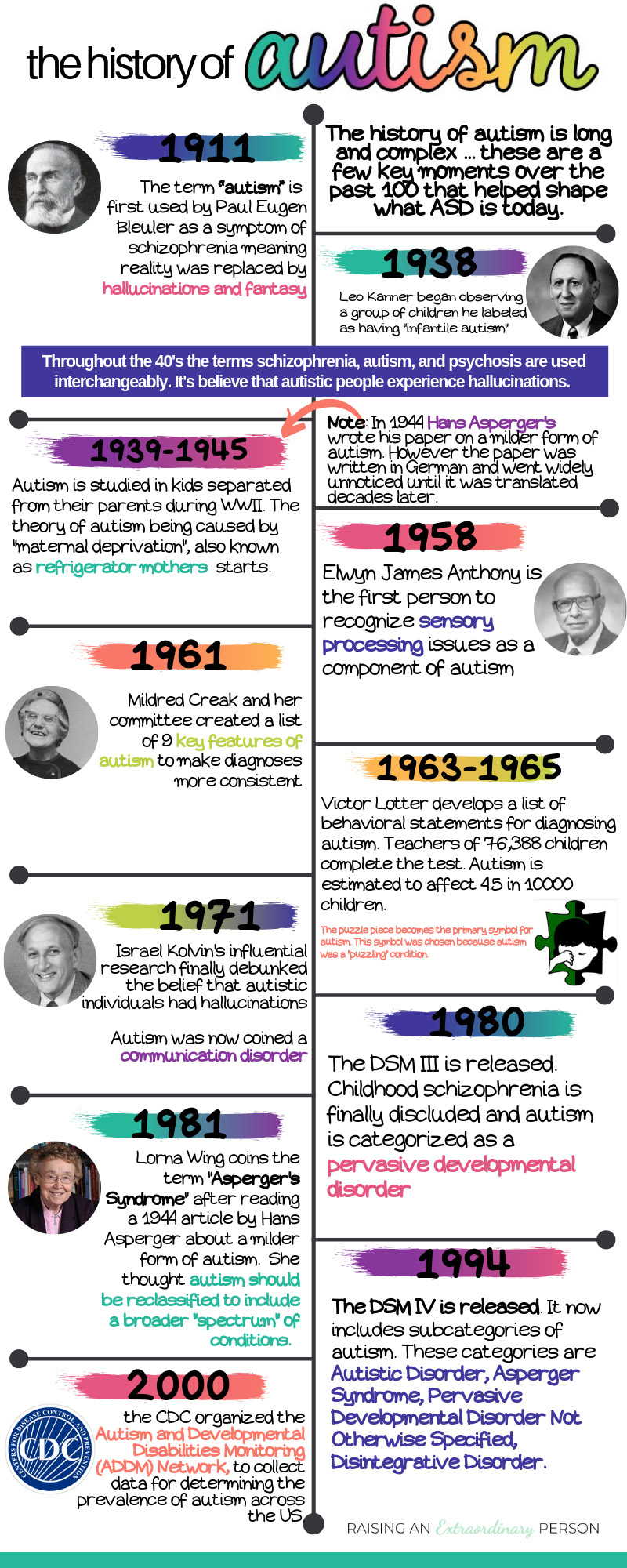
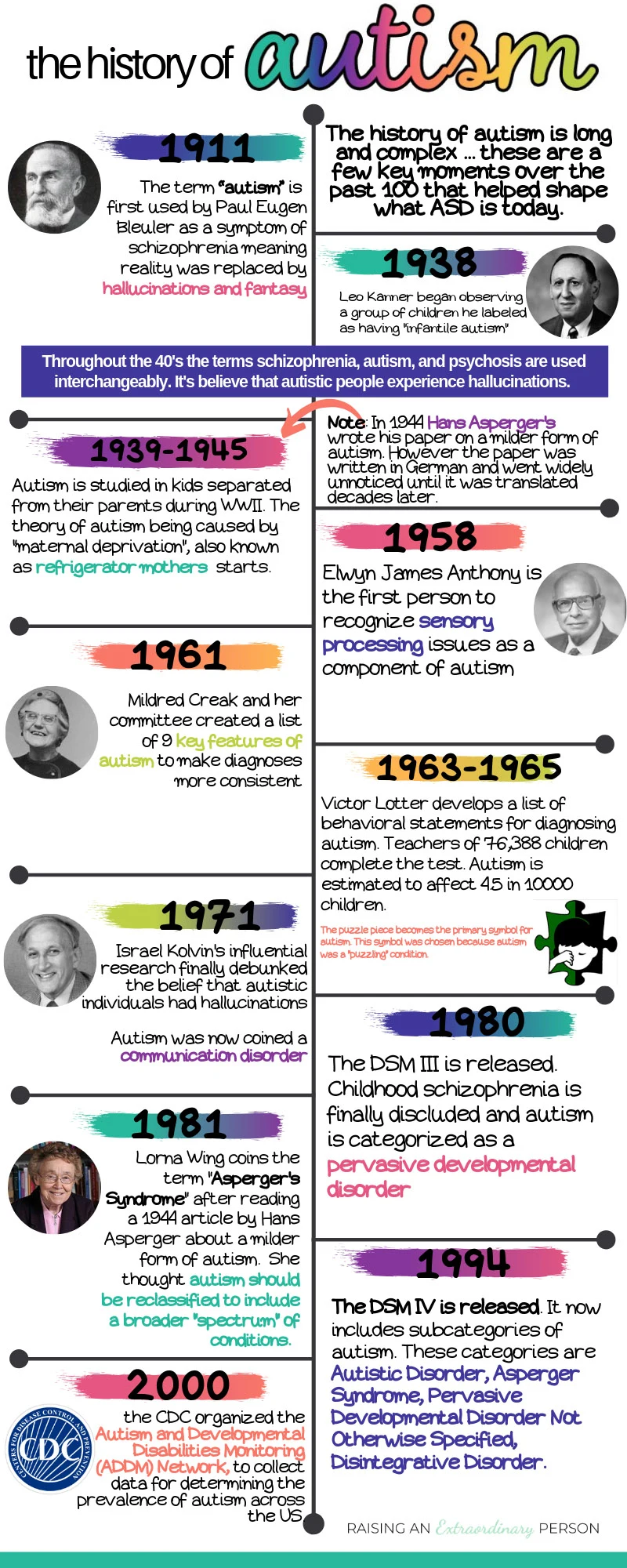
The term “autism” was first used by psychiatrist Paul Eugen Bleuler in 1911. However, he used the term to describe the introspective symptoms of adults with schizophrenia. He defined autism as “wishes to avoid unsatisfying realities and replace them with fantasies and hallucinations.”
1920-1950
In the 1920s, Jean Piaget published an article where he theorized that before babies learn to speak, their pre-verbal thoughts consist of only visual imagery, and so they cannot make logical conclusions about the world around them. He called this pre-verbal thought period in infants “infantile autism.”
From there, a doctor named Leo Kanner began observing a group of children who were previously diagnosed with “mental retardation.” He observed them from 1938 to 1942. He noticed that these children had difficulty developing speech and did not socially interact with their peers during this time. He also noted that these children engaged in ritualized and/or repetitive behaviors to the exclusion of other activities.
Additionally, these children had difficulties with transitions and did not like changes in their routines or schedules. Some of them also experienced regressions in their functioning over time, losing skills that they had established previously.
Kanner described these children as having “infantile autism” in his work, published in 1943. Using the same term as Jean Piaget, but to explain these children’s thinking beyond infantry.
Essentially, there was significant debate throughout the ’40s regarding what autism is. As a result, diagnoses of autism, psychosis, and schizophrenia were often interchangeable throughout the ’40s and ’50s
During the second world war, the children these psychologists studied often were unaccompanied in wartime nurseries in London. This was when the theory of “maternal deprivation” or “refrigerator parents” began, which was a theory that a lack of parental love and affection causes autism.
1960-1970
In 1958, Elwyn James Anthony began his work to categorize which areas of development autism consistently impacted. He also worked to define what “normal” child development looked like. Anthony was the first to note sensory processing issues along with autism, what he called “raised sensory thresholds.”
Many child psychologists started challenging Bleuler’s original definition. So, by the mid-’60s, doctors were using the term autism to describe what was basically the exact opposite of the original definition, believing it to be “a complete lack of an unconscious symbolic life.”
In 1961, Mildred Creak and a committee of 13 multidisciplinary medical professionals created a list of 9 key features of “schizophrenic syndrome in childhood” (describing what we now know is autism). She believed that if everyone could agree on key diagnostic features, it would be much easier to study, understand, and recognize the syndrome.
The Key Features of Autism
The committee agreed on the following key features:
- gross and sustained impairment of emotional relationships with people
- apparent unawareness of his own personal identity
- pathological preoccupation with particular objects
- sustained resistance to change in the environment
- abnormal perceptual experience
- acute, excessive and seemingly illogical anxiety
- Loss of speech, or never acquired
- distortion in motility patterns
- a background of serious retardation in which islets of normal, near normal, or exceptional intellectual function or skill may appear
Many mental institutions closed in the 60s after Britain passed The Mental Health Act. So, Botleys Park Hospital for the mentally handicapped in Chertsey selected children they considered autistic, as per Creaks 9 key features, and then categorized them based on IQ tests.
They then tried to test Anthony’s theories of sensory processing by using behavioral tests. Children were rewarded for correctly responding to tactile, auditory, and visual stimulation. The results of these tests suggested that ‘autistic’ children are more likely to respond to tactile and visual stimulation than auditory stimulation. However, they could learn to respond to sound by using rewards. This research was the basis and beginning stages of ABA therapy.
Leading up to the creation of the Diagnostic Statistical Manual, in 1965 psychologist Victor Lotter developed a list of behavioral statements for identifying and diagnosing autism. Teachers of 76,388 children between the ages of 8 and 10 attending schools in the Middlesex area completed the test. Children identified by teachers were then further assessed to confirm their autism.
Table by Victor Lotter, ‘Mean percentage scores on 24 behavior items’ (Lotter, 1966).
Lotter believed this was sufficient data to diagnose autism, which was considered a behavioral condition at the time. He noted the initial prevalence of autism within a population of 4.5 in 10,000.
1970- 1980
This occurred in 1971 and from there, researchers began focusing on how autism impacts language. Ultimately, the influential work of Israel Kolvin, from the Nuffield Child Psychiatry Unit in Newcastle, eliminated the belief that children with autism had hallucinations. This is when autism was coined a communication disorder.
These language differences, thought to be caused by a cognitive deficit at the time, became a defining feature of autism.
In the late 70s, Rutter and Eric Schloper (who took over for Kanner) worked hard to create a new style of thinking about childhood development, and they saw the categories of ‘autism’ as central to this. At the same time, they began excluding ‘psychosis’ and ‘schizophrenia’ from child psychology. This was a major turning point.
1980’s
In 1980 the 3rd edition of the Diagnostic Statistical Manual was released, which completely excluded “childhood schizophrenia”. It also removed “autism” as part of the diagnostic criteria for adult schizophrenia. Finally and officially separating the two diagnoses into completely separate categories.
Autism was now under “Pervasive Developmental Disorders”.
The new understanding of autism and the neurodevelopmental aspects of the disorder expanded the diagnostic criteria. Now, ‘Impairments of reciprocal social interaction’ were reported to occur in 21.2 of every 10,000 children in the area studied, of whom 4.9 presented with a history of ‘typical autism.’
This is when autism began progressing to the spectrum disorder we know today. Psychiatrists Lorna Wing and Judith Gould proposed that autism should be reclassified as a ‘wider group of conditions which have, in common, impairment of the development of social interaction, communication, and imagination’.
In 1981, she coined the term ‘Asperger’s syndrome’ after reclaiming a 1944 article on autism by Hans Asperger. Although Asperger’s Syndrome was not in the DSM until its 4th edition in 1994. Note: Asperger’s syndrome has since been removed from DSM upon the release of the DSM V in 2013.
The meaning of autism had transformed and increasing numbers of children could now be defined by these new classificatory criteria.
1990’s
In 1991, autism was officially recognized as a special education category. This meant public schools began recognizing autistic children and providing them with specialized services.
The DSM IV, released in 1994, now included subcategories of autism. These categories are Autistic Disorder, Asperger Syndrome, Pervasive Developmental Disorder Not Otherwise Specified, Disintegrative Disorder.
Symptoms were divided into three areas: social reciprocity, communicative intent, restricted and repetitive behaviors.
Increased awareness meant that people previously diagnosed with childhood schizophrenia or minimal brain damage were recognized as having autism all along. It was now believed that roughly 1 in 2500 children were autistic.
During the ’90s professionals often used an intervention known as “holding therapy”. This involved restraining autistic children and forcing them to engage in various social behaviors, for example, making eye contact.
Unfortunately, throughout the ’90s, funding largely went towards determining the causes of autism rather than working on therapies and other treatments that could help autistic individuals. As a result, the interventions used often did more harm than good.
2000s
In 2000, the CDC organized the Autism and Developmental Disabilities Monitoring (ADDM) Network, to collect data for determining the prevalence of autism across the US.
Then, in 2006, they released their first report which indicated that 1 in 150 children are autistic. By 2009, the CDC reported that number to be 1 in 110 children.
2010 – Today
Scientists begin to understand the genetic components of autism. In a 2011 study, 65 gene variations were discovered in connection to autism. Scientists determined, through genome sequencing, that approximately 5% of autism cases are from “de novo mutations.” These are mutations present for the first time in one family member due to a mutation in a germ cell (egg or sperm) of one of the parents or in the fertilized egg itself.
A study published in 2015 identified another 102 gene mutations associated with ASD.
In 2013, the DSM V was released. This newest version of the diagnostic statistical manual removed the subcategories of autism (Asperger’s, PDD-NOS, Rett’s), and now all diagnoses are called Autism Spectrum Disorder (ASD). Diagnosis now comes with an accompanying level which indicates the amount of extra support the individual needs.
Autism Diagnostic Criteria
There’s a lot of information here that sounds very clinical, but the reason is to show you everything considered from a clinical standpoint when making an autism diagnosis.
Diagnostic Statistical Manual V
Your child’s diagnosis is based on the criteria outlined in the Diagnostic Statistical Manual V (DSM V). In order to receive a diagnosis of “Autism Spectrum Disorder” individuals must meet the criteria in the following areas:
- Persistent deficits in social communication and social interaction across multiple contexts
- Restricted, repetitive patterns of behavior, interests, or activities. At Least two repetitive motor movements, insistence on sameness, restricted fixated interests, hyper or hypoactivity to sensory input.
- Symptoms are present in early childhood and more noticeable when social demands begin to exceed capacity (such as starting school or daycare)
- Symptoms limit or impair daily functioning
Components Involved in an Autism Assessment
Assessment and diagnosis of ASD involve gathering and analyzing information on the individual’s development. Contributions that provide an overall profile of the individual may come from
- educators
- parents/guardians
- board based ASD specialists
- speech-language pathologists
- occupational therapists
- psychologists
- other medical professionals
- early interventionists
- pre-school or day-care personnel
The person performing the assessment will also spend time with your child, one on one, doing various activities. This allows them to gauge your child’s development across various domains and observe first hand any indicators that your child is autistic.+
Additional Information In Your Diagnosis
Your child’s ASD diagnosis will specify:
- With or without accompanying intellectual impairment
- With or without accompanying language impairment
- Association with a known medical, genetic, or environmental factor
Your child’s diagnosis may also specify a level:
- 1: Requiring very substantial support
- 2: Requiring substantial support
- 3: Requiring support
This indicates the level of support/intervention required for social communication and repetitive/restricted behaviors
It may also indicate whether or not there are any other coexisting conditions.
The PDF file below explains each of the criteria in more depth with specific examples for each.
Signs & Symptoms of Autism


The signs and symptoms of autism vary widely. You should always consult a doctor if you have any concerns about your child’s development. The following are some common signs of ASD in early childhood:
- Doesn’t respond to his or her name or to the sound of a familiar voice
- Doesn’t follow objects visually, or follow your gesture when you point
- Does not use communicative gestures, for example pointing or waving.
- Lack of pretend play, or when they do play pretend they reenact things they saw on TV or from other kids.
- Cannot follow directions that have more than one or two steps
- Doesn’t make noises to get your attention
- Speaks with an abnormal tone of voice, odd rhythm, or pitch. For example, everything they say sounds like they’re asking a question.
- Doesn’t initiate or respond to cuddling or reach out to be picked up.
- Doesn’t imitate your movements or facial expressions.
- Reacts unusually to sounds, smells, textures, or sights.
- Seems as though they don’t notice or care if you hurt yourself or experience discomfort
- Doesn’t play with other children. May play beside them but with little interaction.
Since the signs of autism can present differently in different children, they aren’t always apparent. Read about the 9 signs of high-functioning autism that I missed.
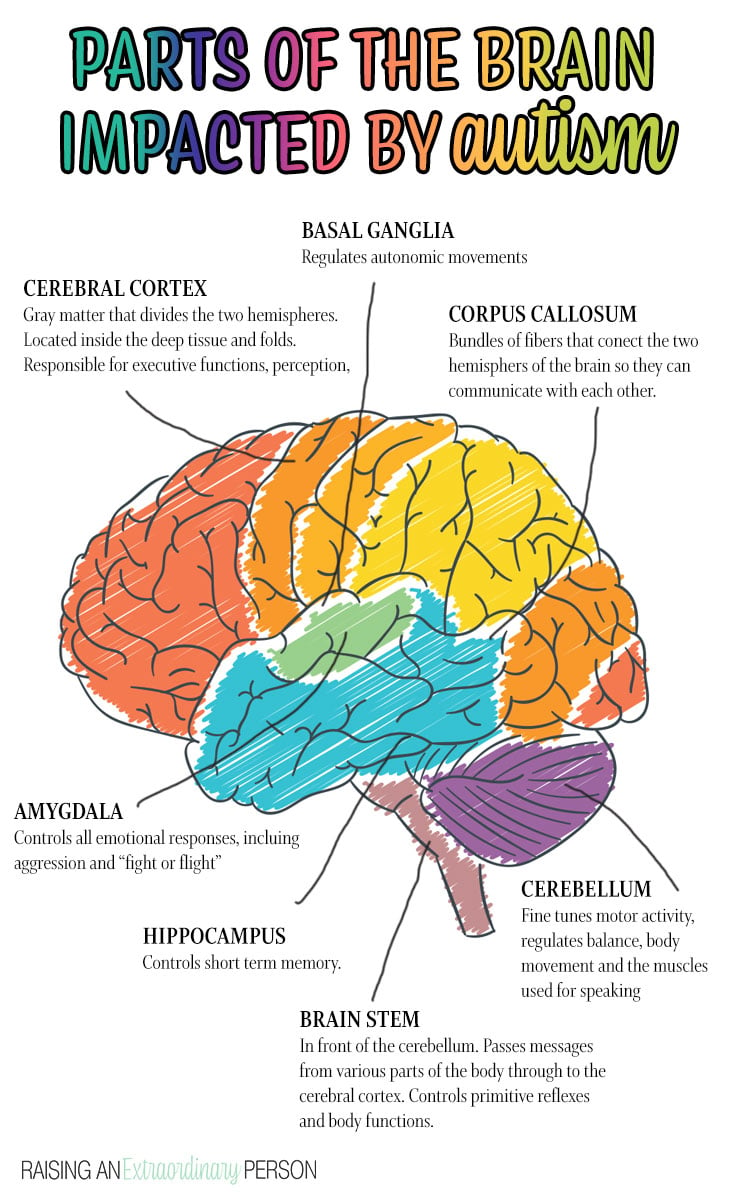
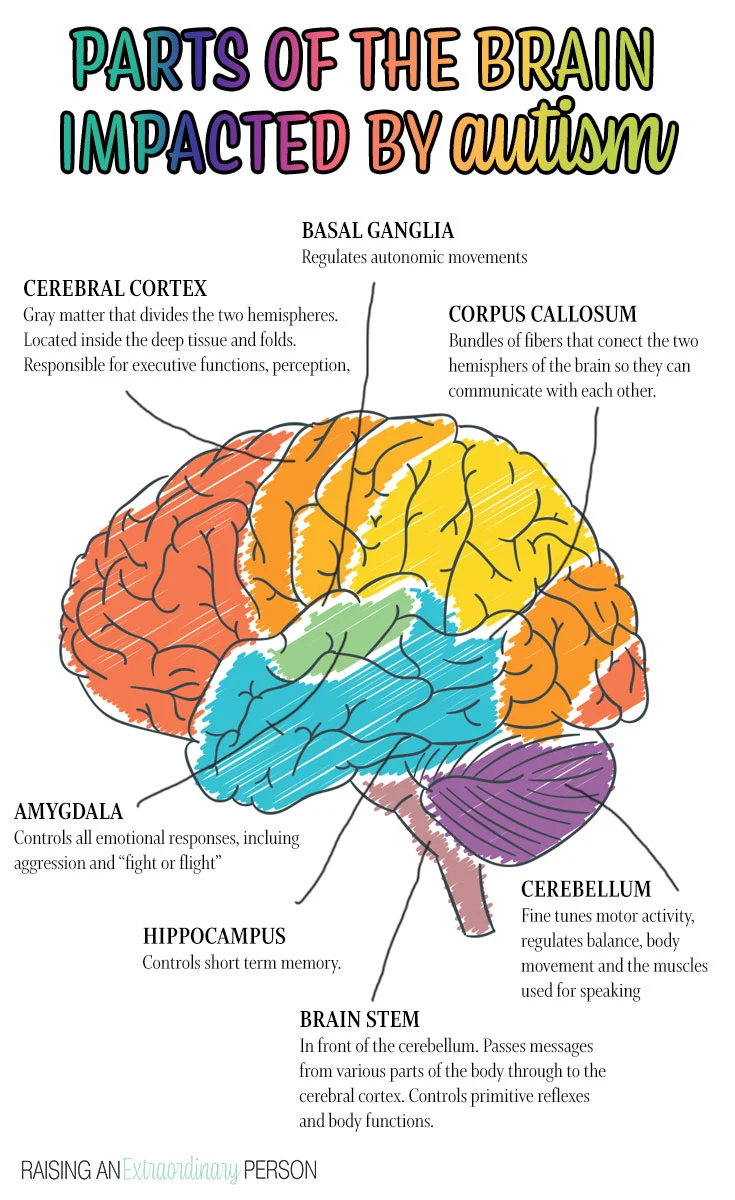
Parts of the Brain Affected By Autism
Because ASD is a brain-based disorder, it affects several parts of the brain. It influences thinking, learning, interpretation of sensory input, and being with others.
How areas of the brain communicate with each other is also affected. As a result, sensory processing and motor skills, executive functions, emotional regulation, and communication skills are all affected.
Autism Statistics & Prevalence
According to the Autism & Developmental Disabilities Monitoring Network, ASD affects 1 in 59 people (data from 2014) (read article)
However, results from a 2014 parent survey state that 1 in 45 children ages 3-17 currently has an autism diagnosis.
Autism is the fastest-growing developmental disorder. According to the University of Calgary, there’s been an 1148% increase in the last ten years.
Boys are 4-5 times more likely to receive an autism diagnosis than girls. Although it’s thought to affect boys and girls equally, the symptoms present differently in girls, making it more challenging to diagnose.
The median age of diagnosis is 4-5 years old (CDC, 2008)
Autism Prevalence As Per The CDC
| YEAR | BIRTH YEAR | PREVALENCE OF AUTISM |
|---|---|---|
| 2000 | 1992 | 1 in150 |
| 2004 | 1996 | 1 in 125 |
| 2006 | 1998 | 1 in 110 |
| 2008 | 2000 | 1 in 88 |
| 2010 | 2002 | 1 in 68 |
| 2014 | 2006 | 1 in 59 |
| 2016 | 2008 | 1 in 54 |
Intellectual Disability
Experts once thought that nearly everyone with autism also had cognitive deficits, but we now know that is not the case.
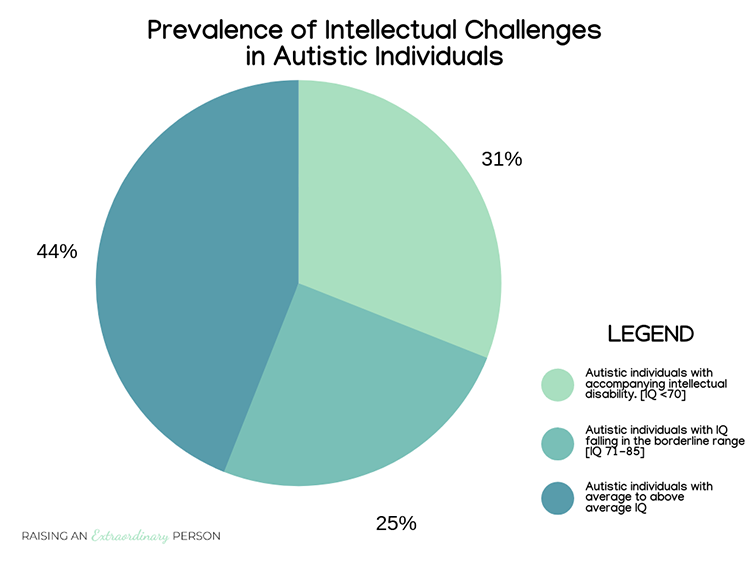
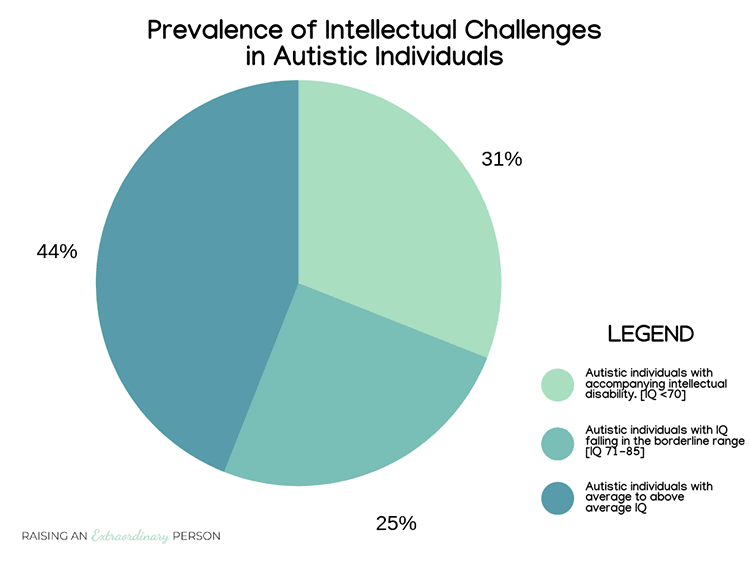
Note that this chart is based on IQ data from people with ASD. Although IQ tests have existed for a long time, they may not accurately define people’s intelligence with communication challenges because much of the testing requires communication. Therefore, the number of people with below-average intelligence is probably even lower; they don’t have the communication skills to show it in standardized test scores like this one.
Comorbities
Children with autism often have other coexisting conditions as well.
There is still a lot to learn and discover about autism. In the past, negative associations of autism led to poor treatment and interventions for people with autism. It’s essential to continue looking at autism more positively, noting the individual’s strengths and challenges.
Every individual with ASD has unique strengths, interests, talents, and areas that challenge them.
Understanding these strengths, interests, and talents on a person-to-person basis can help individualize interventions and strategies used to teach new skills and improve areas where challenges exist.
Sensory Diet Activities for Your Child's Unique Sensory Profile
Tuesday 10th of December 2019
[…] Plus, 98% of children with autism have sensory issues. It’s one of the hallmark symptoms of Autism Spectrum Disorder. […]
9 Signs of High Functioning Autism That I Missed -
Thursday 24th of October 2019
[…] This is just a basic overview of what autism is if you aren’t familiar with it. If you wish to learn more, you can read in-depth about the history of autism, facts and statistic, s… […]
8 Awesome "Autism Traits" · Autism Resources for Parents
Sunday 1st of September 2019
[…] unfortunate, but the diagnostic criteria for Autism Spectrum Disorder focuses only on the deficits associated with autism. This creates such a negative picture of such […]
Pam
Wednesday 22nd of May 2019
We are trying to get our 10 year old grandson tested for autism, the NHS waiting list is years long and we thought about going private but that also has a very long waiting list. We don't know where to go next. Our son who is 43 has been diagnosed with it as well, but cannot get help. Do you have any suggestions?
Nicole Day
Wednesday 22nd of May 2019
It's a very long wait here as well. My advice would be to research evidence-based strategies used by schools and special programs for children with autism and begin using them yourself to the best of your ability, to help him out. Even if it turns out that he's not autistic if he's struggling with some of the same challenges, the strategies are designed to help. There's a lot of information here on the blog but lots of great resources out there too. If you have any specific questions feel free to get in touch and I can try to point you in the right direction.